EUROLINE
positive control serum: IgG, human, 100x concentrated
for DL 1300-X G
EUROASSAY
AMA M2, LKM-1, SLA/LP
EUROASSAY strip
with antigens
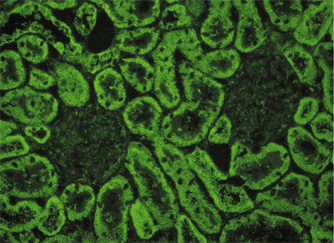
IIFT
Liver Mosaic 1
liver-kidney microsomes (LKM), ANA
mitochondria (AMA), LKM
2 BIOCHIPs per field:
liver
kidney
rat
rat
EUROLINE
Liver Profile 2
(AMA M2, M2-3E, LKM-1, LC-1, SLA/LP separately)
EUROLINE
IIFT
Liver Sreen 1
mitochondria (AMA), LKM
soluble liver antigen/
liver-pancreas antigen (SLA/LP)
LKM, ANA
smooth muscles (ASMA)
4 BIOCHIPs per field:
kidney
transfected cells
liver
stomach
rat
EU 90
rat
rat
EUROLINE
Liver Profile
(AMA M2, LKM-1, LC-1, SLA/LP separately)
EUROLINE
EUROASSAY
Liver Profile
AMA M2, LKM-1, LC-1, SLA/LP
EUROASSAY strip
with antigens
EUROLINE
Autoimmune Liver Diseases
(AMA M2, M2-3E, Sp100, PML, gp210,
LKM-1, LC-1, SLA/LP, Ro-52 separately)
EUROLINE
EUROLINE
Autoimmune Liver Diseases 14 Ag
(AMA-M2, M2-3E, Sp100, PML, gp210,
LKM-1, LC-1, SLA/LP, SS-A, Ro-52, Scl-70,
CENP A, CENP B, PGDH separately)
EUROLINE
IIFT
Liver Mosaic 8
liver antigens, cell nuclei (ANA)
F-actin
cell nuclei (ANA)
LKM, ANA
mitochondria (AMA), LKM
smooth muscles (ASMA)
6 BIOCHIPs per field:
liver
VSM47
HEp-2 cells
liver
kidney
stomach
monkey
rat
human
rat
rat
rat
EUROLINE
Autoimmune Liver Diseases 9 Ag plus F-Actin
(AMA-M2, M2-3E, Sp100, PML, gp210,
LKM-1, LC-1, SLA/LP, F-Aktin und Ro-52)
EUROLINE
IIFT
Liver Mosaic 9
mitochondria (AMA), LKM
LKM, ANA
smooth muscles (ASMA)
F-actin
4 BIOCHIPs per field:
kidney
liver
stomach
VSM47
rat
rat
rat
rat
IIFT
Autoimmune liver diseases Screen 9
EUROPattern
mitochondria (AMA), LKM
LKM, ANA
smooth muscles (ASMA)
F-actin
4 BIOCHIPs per field:
kidney
liver
stomach
VSM47
rat
rat
rat
rat
IIFT
mitochondria (AMA)
kidney
rat
ChLIA
IDS AMA (M2) 1
antigenic coated magnetic particles
EUROASSAY
AMA Profile
(AMA M2, M4, M9 separately)
EUROASSAY strip
with antigens
EUROLINE
AMA-Profile EUROLINE
(separate: AMA-M2, M2-3E, M4, M9)
EUROLINE
IIFT
mitochondria (AMA)
smooth muscles (ASMA)
kidney
stomach
(2 BIOCHIPs per field)
rat
rat
IIFT
AMA/ASMA IIFT (KR/SR) EUROPattern
mitochondria (AMA)
smooth muscles (ASMA)
2 BIOCHIPs per field:
kidney
stomach
rat
rat
IIFT
EUROPLUS
mitochondria (AMA)
smooth muscles (ASMA)
cell nuclei (ANA)
M2 antigen
4 BIOCHIPs per field:
kidney
stomach
HEp-2 cells
M2 BIOCHIPs
rat
rat
human
IIFT
antibodies against mitochondria
(AMA M2 control; associated with PBC)
ELISA
AMA M2-3E
antigen-coated
microplate wells
IIFT
Mosaic Basic Profile 1
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
3 BIOCHIPs per field:
HEp-2 cells
kidney
stomach
human
rat
rat
IIFT
Mosaic Basic Profile 2
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
3 BIOCHIPs per field:
liver
kidney
stomach
rat
rat
rat
IIFT
Mosaic Basic Profile 2 EUROPattern
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
3 BIOCHIPs per field:
liver
kidney
stomach
rat
rat
rat
IIFT
Mosaic Basic Profile 3
cell nuclei (ANA)
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-2 cells
liver
kidney
stomach
human
monkey
rat
rat
IIFT
Mosaic Basic Profile 3A
cell nuclei (ANA)
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
monkey
rat
rat
IIFT
Mosaic Basic Profile 3A EUROPattern
cell nuclei (ANA) EUROPattern
cell nuclei (ANA)
mitochondria (AMA)
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
monkey
rat
rat
IIFT
Mosaic Basic Profile 13B
cell nuclei (ANA)
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-2 cells
liver
kidney
stomach
human
rat
rat
rat
IIFT
Mosaic Basic Profile 13B EUROPattern
cell nuclei (ANA), EUROPattern
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-2 cells
liver
kidney
stomach
human
rat
rat
rat
IIFT
Mosaic Basic Profile 3C
cell nuclei (ANA)
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
rat
rat
rat
IIFT
Mosaic Basic Profile 3C EUROPattern
cell nuclei (ANA), EUROPattern
cell nuclei (ANA), LKM
mitochondria (AMA), LKM
smooth muscles (ASMA)
4 BIOCHIPs per field:
HEp-20-10 cells
liver
kidney
stomach
human
rat
rat
rat